Ocular Hypertension (OHT) refers to consistently elevated intraocular pressure (IOP) without clinical signs of glaucomatous optic neuropathy or visual field loss. However, if left unmanaged, it can progress to Chronic Open Angle Glaucoma (COAG) and cause irreversible vision damage.
The primary goal in managing OHT is to reduce IOP and prevent progression to glaucoma — particularly in those at high risk of visual impairment during their lifetime.
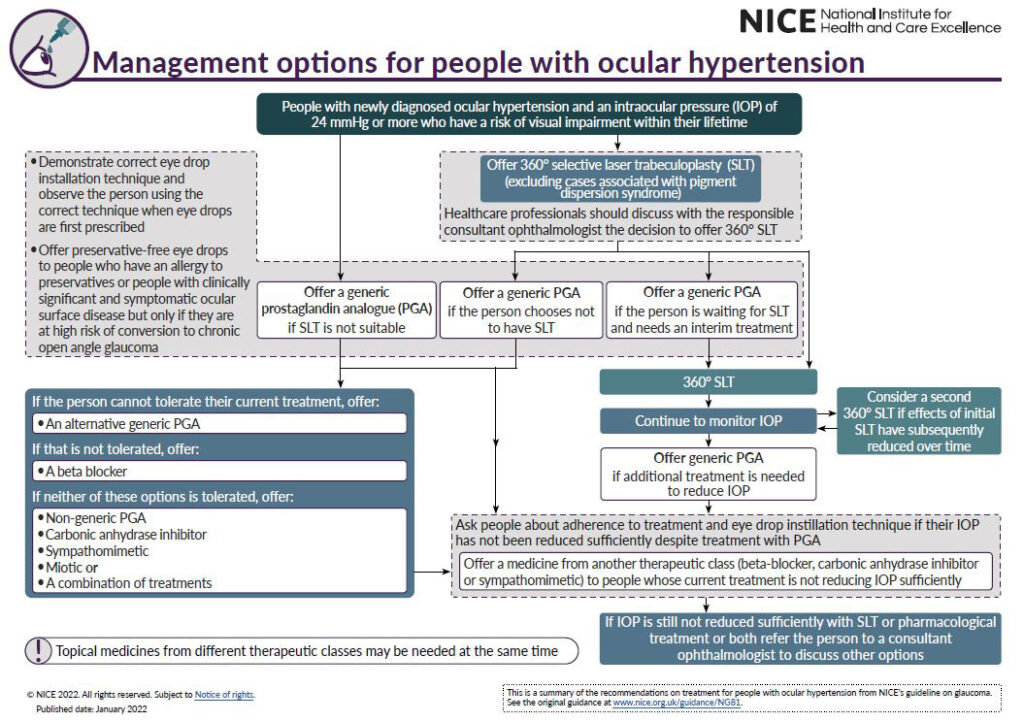
🔑 Key Management Principles for OHT
The NICE guidelines recommend a stepwise, risk-based approach, starting with laser or medication, followed by ongoing monitoring, and escalating as needed.
1️⃣ First-Line: 360° Selective Laser Trabeculoplasty (SLT)
- For newly diagnosed OHT, especially when IOP ≥ 24 mmHg and the individual is at risk of lifetime visual impairment, 360° SLT is the first-line intervention.
- The decision should be discussed with the consultant ophthalmologist, ensuring informed patient choice.
2️⃣ Pharmacological Management: Generic PGAs and Beyond
If SLT is not chosen, not suitable, or the patient is awaiting treatment, start with a generic prostaglandin analogue (PGA).
📌 If PGA is:
- Not tolerated: Offer an alternative generic PGA → then a beta-blocker.
- Still not tolerated: Consider non-generic PGAs, carbonic anhydrase inhibitors, sympathomimetics, miotics, or combinations.
📌 If IOP remains high despite one medicine:
- Add or switch to another class (e.g., combine PGA with beta-blocker or CAI).
💧 Preservative-free drops should be considered for those with ocular surface disease or allergy to preservatives, especially if at high risk of conversion to glaucoma.
3️⃣ Adherence & Technique: A Crucial Step
Before escalating treatment:
- Demonstrate and observe proper eye drop instillation.
- Ask about adherence, especially if IOP is not adequately reduced.
👁️ Poor drop technique or non-compliance is often the hidden cause of treatment failure.
4️⃣ Further Interventions
A second SLT may be considered if the first treatment’s effect has diminished.
- If IOP is still not controlled, refer to a consultant ophthalmologist to explore other options like surgical interventions or advanced medications.
5️⃣ Continuous Monitoring: The Long-Term Pillar
Management of OHT doesn’t stop with starting treatment. Regular follow-ups are essential to:
- Monitor IOP trends
- Reassess conversion risk to COAG
- Adjust therapy or escalate when required
📝 Final Thoughts
NICE guidelines emphasize that the earlier and more appropriately we intervene, the better the chances of preventing glaucomatous damage.
📌 Whether you choose SLT or pharmacological therapy, the focus remains the same:
👉 Individualized care, patient education, adherence, and lifelong monitoring.
🔗 Stay tuned to EyeCapsule for more evidence-based ophthalmology content and FRCOphth-focused guidance.